Translingual-induced neurostimulation (TLNS) employs neural mechanisms that may compensate for abnormal activity of corticospinal pathways involved in regulating movement and coordination.
The tongue, which has a large cortical representation, is innervated in its front two-thirds by branches of the trigeminal and facial nerves with direct connections to the brainstem. Clinical evidence suggests that PoNS Therapy® (PoNS device plus physical therapy) can exert neuromodulation effects by the translingual stimulation of the lingual nerve (trigeminal nerve branch) and chorda tympani (facial nerve branch).
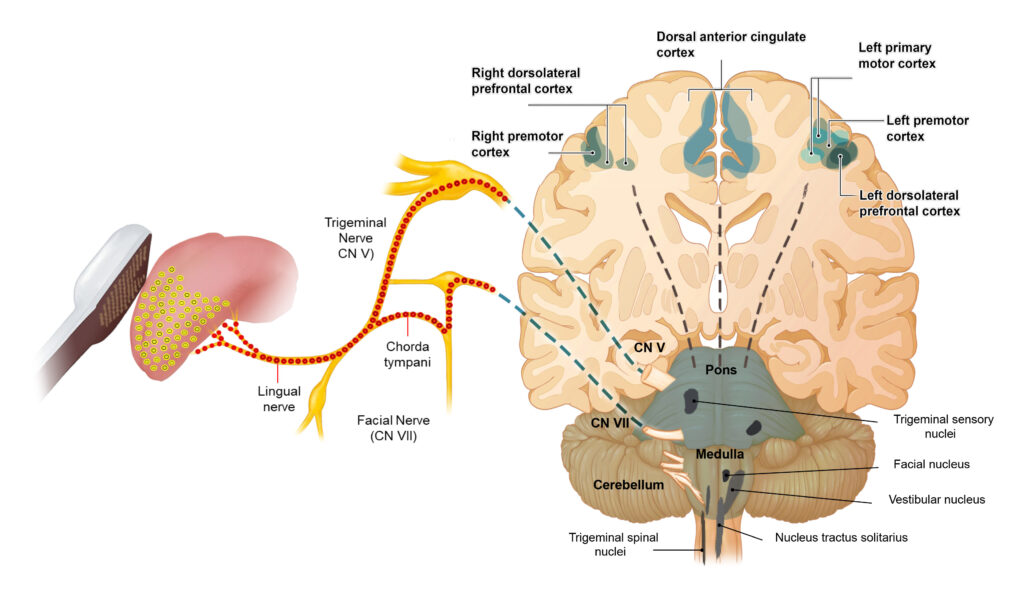
These cranial nerves have direct connections with specific areas of the brainstem (in the pons variolii and the medulla). Translingual stimulation promotes activation of mechanisms involved in neuromodulation of signaling pathways from these brainstem areas to target regions in the cerebral cortex including the left motor cortex, the bilateral anterior cingulate and dorsolateral prefrontal cortex areas that may contribute to regulate functional and cognitive mechanisms of movement and balance control.
Sustained PoNS-induced neuromodulation of these cortical areas is believed to promote adaptive changes leading to the development of new neurite/axonal networks to replace/repair impaired corticospinal tract pathways that deliver the signal to the spinal cord.
Consistent application of PoNS Therapy, over 14 weeks, is likely to consolidate these neuroplasticity mechanisms, which may compensate for the loss/decrease of function and be ultimately responsible for the therapeutic effects over the treatment period.